EXPLORE THE NEUROSCIENCE OF EMDR AND SOMATIC BELIEF CHANGE. LEARN HOW BILATERAL STIMULATION UPDATES BODY-HELD TRAUMA BELIEFS STEP BY STEP WITH PROVEN SCIENCE.
CHANGE DEEP BELIEFS WITH EMDR: A STEP-BY-STEP GUIDE
EMDR Eye Movement Desensitization and Reprocessing is one of the most thoroughly researched methods for dismantling traumatic belief systems. What makes it unusual is where it works: not just in the thinking mind, but in the body itself. Beliefs like “I am powerless” or “I am not safe” are not stored as abstract ideas. They live as posture, as breath, as the particular tension across a jaw or the hollow feeling behind a sternum.
This article maps the full eight-phase EMDR protocol through a body-first lens. Each phase is treated as an iterative loop in which the nervous system re-samples a traumatic memory under new conditions, gradually shifting the probability the body assigns to threat versus safety. You will find the neuroscience, a complete step-by-step process guide, a full practitioner session script using Submodality Mapping Across, a somatic meditation, and honest assessments of what EMDR can and cannot do.
Whether you are a therapist, an NLP practitioner, or someone curious about how lasting belief change actually happens in the body, this is a ground-level map of the territory.
🎯 THE BENEFITS OF EMDR AND SOMATIC BELIEF CHANGE
“I went in thinking my beliefs lived in my head. I came out realizing my entire skeleton had opinions.” - Anonymous
EMDR produces changes that talk therapy alone rarely reaches. The benefits are not merely psychological they are registered at the level of muscle tone, breathing patterns, and visceral sensation, because that is where the belief was stored in the first place.
Relief from chronic somatic arousal. Many people with embedded trauma beliefs live with a background hum of tension a braced quality in the shoulders, a shallow breath, a gut that rarely settles. After successful EMDR processing, this somatic baseline shifts. The body stops organizing itself around a threat that no longer exists. You may notice this as a felt release, a sense of dropping weight you had forgotten you were carrying, or simply that you can breathe all the way down into your belly without effort.
Rapid updating of the negative cognition. The Validity of Cognition (VoC) scale measures how much the body believes a positive statement. A belief like “I have choices now” may begin a session at VoC 2 the body barely registers it as true and end at VoC 7. This is not intellectual agreement. It is the somatic certainty that comes when a new belief has been installed at the level where the old one lived.
Reorganization of traumatic memory. Trauma memories are often stored as fragmented, sensory snapshots a smell, a flash of image, a sudden terror without context. Research published in Frontiers in Psychology found that EMDR facilitates the shift of such memories from fragmented sensory encoding toward coherent autobiographical narrative. The memory remains, but it loses its charge. It moves from happening now to something that happened then.
Neurological restructuring. Brain imaging studies have documented increases in grey matter volume in the left parahippocampal gyrus a region central to memory integration and reductions in thalamic overactivation after successful EMDR treatment. In one study, PTSD diagnosis was eliminated in sixteen of nineteen patients. These are not subjective reports. They are visible on scans.
Somatic expansion and resource access. One of the quieter benefits is the reclamation of body sensations previously associated only with threat. Sensations like warmth in the chest, openness in the throat, or steadiness in the legs which may have been absent or numbed for years begin to return as resources rather than warnings.
Better decisions under pressure. When the body is no longer misreading present-moment stimuli through the lens of old trauma, perceptual accuracy improves. The gut signal becomes cleaner. Choices feel less like emergencies and more like genuine options.
🏛️ ORIGINS OF EMDR ACROSS CULTURES AND HISTORY
The formal origin of EMDR is precisely dated. In 1987, American psychologist Francine Shapiro was walking in a park when she noticed that distressing thoughts seemed to lose their intensity as her eyes moved back and forth following the movement of light through leaves. She began experimenting systematically and published her initial findings in 1989. The protocol evolved rapidly through the 1990s, gaining endorsement from the American Psychiatric Association and the World Health Organization as a frontline treatment for PTSD.
What is less commonly noted is that the underlying mechanics using rhythmic bilateral movement to shift the nervous system’s relationship to memory have analogues across many older traditions.
Shamanic drumming and bilateral rhythm. Shamanic traditions across cultures use repetitive bilateral percussion drumbeats that alternate in a steady left-right pattern to shift consciousness and facilitate what practitioners describe as the release of fixed patterns. The mechanism, from a neuroscience perspective, may overlap with what bilateral stimulation accomplishes in EMDR: taxing working memory while simultaneously activating present-moment sensory input, disrupting the fixity of a looped internal experience.
EMDR and REM sleep. The eye movements used in classical EMDR closely resemble those that occur during Rapid Eye Movement sleep, the phase associated with emotional memory consolidation. Sleep researchers have proposed that one function of REM is precisely the kind of adaptive memory processing EMDR attempts to accelerate: integrating emotionally charged experience into a broader autobiographical context where it no longer triggers alarm.
Somatic psychology traditions. Wilhelm Reich’s work in the 1930s proposed that traumatic experience is held in the body as chronic muscular tension, which he called “character armor.” Peter Levine’s Somatic Experiencing, developed decades later, emphasizes completing interrupted threat-response cycles through body sensation. EMDR integrates with these traditions naturally because it requires tracking body sensation throughout the body scan at Phase 6 is, in essence, a somatic verification that the belief change has fully landed.
NLP and submodality work. Richard Bandler and John Grinder’s development of Neuro-Linguistic Programming in the 1970s and 1980s demonstrated that the structural qualities of internal representations the brightness, location, size, and movement of mental images could be systematically altered to change their emotional charge. EMDR’s bilateral stimulation can be understood as an accelerated method for accomplishing the same reorganization, using sensory rhythm rather than deliberate submodality manipulation to generate the necessary processing conditions.
📜 PRINCIPLES OF EMDR AND SOMATIC BELIEF CHANGE
Principle 1: The belief lives in the body, not the mind
When a person says “I know intellectually I’m safe, but I don’t feel it,” they are describing the gap between cognitive understanding and somatic encoding. The belief that matters the one that governs behavior, colors perception, and shapes posture is the one the body holds. EMDR targets the somatic layer directly. Until the body updates, intellectual reframing produces no durable change.
Notice where you carry your version of “I am not enough.” Is it a tightening across the chest? A subtle pull forward of the head? A constriction at the base of the throat? That location is the actual address of the belief.
Principle 2: Trauma freezes the probability distribution
The nervous system functions, broadly, as a prediction engine. It continuously evaluates incoming sensory data against stored models of the world to generate the most probable interpretation. Under trauma, this system becomes stuck: the probability assigned to threat remains pathologically high regardless of present circumstances, because the memory that established it was never properly integrated.
EMDR works by exposing the nervous system to the traumatic memory under conditions bilateral stimulation, dual attention that interrupt the freeze. Each bilateral stimulation set is a re-sampling event that gradually shifts the probability distribution from threat-dominant to adaptive.
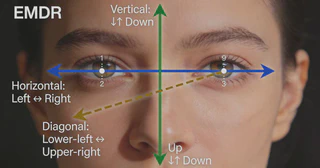
When you hold a traumatic image in mind while following bilateral eye movements or bilateral taps, two things happen simultaneously: the memory activates, and present-moment sensory information floods in from both hemispheres. The brain’s predictive model was not expecting this combination. The discrepancy between what it predicted (distress) and what is actually arriving (present-moment rhythm, the therapist’s calm presence, the feel of the chair) constitutes a prediction error the neurological signal that updates the model.
Over many sets, the model updates. The memory no longer predicts the same alarm.
Principle 4: The body scan is a verification step, not a formality
A belief change that reaches only the cognitive level will revert under stress. The body scan at Phase 6 exists because somatic encoding and cognitive encoding are separate systems. You can genuinely update the thought and still have residual charge stored in the gut, the jaw, or the base of the spine. Only when the body returns neutral no tension, no nausea, no bracing has the update fully installed.
Principle 5: Processing happens between sessions
EMDR does not fully resolve during the session. The brain continues integrating newly processed material overnight, through dreams, and across the days following a session. Clients frequently report that new memories surface, old associations dissolve spontaneously, or they notice behavioral shifts they did not consciously initiate. This is normal. The iterative processing loop runs continuously after each session, extending the work.
Principle 6: The positive cognition must be somatically anchored
The installation phase (Phase 5) is not simply about accepting a more positive thought. The positive cognition “I am safe now,” “I have choices,” “I am worthy of love” must be felt in the body. You are looking for warmth, expansion, steadiness, or a sense of opening. If the positive cognition produces only intellectual neutrality without any felt sense, installation is incomplete.
Principle 7: The therapeutic relationship is part of the protocol
The client’s nervous system does not process in isolation. The regulated nervous system of the therapist their steady breath, their calm attention, their lack of alarm functions as co-regulation throughout the session. The bilateral stimulation accelerates processing; the therapeutic relationship provides the safety container that makes processing possible. Without felt safety, the nervous system will not lower its guard enough to integrate anything.
🗨️ GUIDING CLIENTS IN EMDR
Observation and presence
Position yourself at the client’s side to unobtrusively observe subtle shifts in facial expression, skin tone, and micro-movements of the hands and shoulders. A slight tightening around the eyes or a momentary blanching of the cheeks may signal that processing has accelerated before the client reports anything verbally. Do not interfere with their process or suggest what they should be noticing. Your attention is itself a resource.
Vocal modulation
Use a gentle, melodic, and unhurried tone throughout the session. After each bilateral stimulation set, the instruction “Just notice” or “Take a breath” lands very differently depending on whether it is delivered with calm or with urgency. Let your voice convey that whatever arises is welcome.
Genuine engagement
Demonstrate active interest in the client’s process by listening attentively and supporting their exploratory journey. Resist the pull to reassure prematurely. When a client says “I don’t know what that was,” genuine curiosity “Interesting. Where do you feel that not-knowing in your body?” serves them far better than an anxious attempt to normalize their experience.
Reflective communication
Echo the client’s words and delivery style. If they describe a sensation with a tight, clipped quality “It’s like a fist. Here.” your reflection can match that compressed energy: “A fist. Right there. And what happens when you stay with the fist?” This is not mimicry for its own sake. It communicates that you received exactly what they sent, which deepens trust and safety.
Connecting experience and inquiry
Seamlessly link questions and reflections to the client’s experiences using coordination (and, as, when), ensuring a smooth and empathetic flow throughout the interaction. Rather than “Now tell me your SUD,” try “And as you stay with that, what number comes when you notice how disturbing it feels right now?” The difference is continuity. The client never has to step out of their process to answer an administrative question.
Practical step-by-step guidance for the session:
Introduce bilateral stimulation during the preparation phase, before any memory work. Let the client choose the modality eye movements, taps, or auditory tones and calibrate speed and width to their comfort.
During desensitization, observe the pattern of associations. If a client keeps returning to the same image without movement, this often signals that the body has not yet been invited into the process. Introduce a somatic check: “What do you notice in your body right now?”
If processing stalls or loops, use a cognitive interweave a gentle bridging statement to reintroduce motion: “What would you want that younger version of yourself to know?”
Track SUD and VoC not only through verbal report but through visible somatic markers: unclenching of fists, a visible exhale, a softening of the jaw.
Close every session with a formal body scan and a grounding exercise, regardless of whether processing completed.
💧 EMDR BELIEF CHANGE AXEL MAGNUS SCRIPT BASED ON NLP PRINCIPLES
“I used to think the scary part of EMDR was the eye movements. It turned out the scary part was finding out my body had been running a thirty-year-old software update.” - Anonymous
Technique used: Submodality Mapping Across with Bilateral Stimulation
Preparation building rapport and establishing outcome
Axel Magnus:(Sitting beside the client, voice calm and unhurried) So. You mentioned before we started that there’s a belief that keeps coming back. Something about not being capable. Can you put that in a few words the way it sounds inside when it shows up?
Client: It’s like… “I always mess things up.” Even when things go fine, there’s something waiting for me to prove it true.
Axel Magnus:“I always mess things up.” And when that belief is most active when it’s loudest where do you feel it in your body?
Client:(pauses, hand moving toward chest) Here. Like a compressed weight. Just below my sternum.
Axel Magnus: Like a compressed weight just below the sternum. Good. And if that feeling had a color?
Client: Dark. Brownish grey. Dense.
Axel Magnus: Dense, brownish grey. (writes quietly) And when you imagine a version of you who genuinely knows “I handle things well enough,” where would that feel in your body?
Client:(slight pause, small smile) That one’s lighter. More in my chest, upper chest. Almost warm.
Axel Magnus: Upper chest, warm. Good. That’s where we’re headed. (setting up eye movement track) Before we begin, I want you to know that your only job during processing is to notice whatever comes images, sensations, thoughts, emotions and let them pass through like weather. You don’t have to do anything with them. Just notice and let them move.
Exploration establishing the target memory and baseline measurements
Axel Magnus: I want you to bring to mind the earliest memory you have that’s connected to “I always mess things up.” Don’t look for a specific one just let one come forward.
Client:(several seconds of silence) …There’s one. I’m maybe eight years old. I broke something. My father’s model. He’d been working on it for weeks.
Axel Magnus: Stay with that image. The worst moment. What image comes up most vividly when you hold that memory?
Client: His face when he saw it. His expression. Just… the way he looked at me.
Axel Magnus: His expression when he saw it. And as you hold that image, the negative cognition “I always mess things up” how true does that feel in your body right now, on a scale from one to seven, one being completely false and seven being completely true?
Client: Six. Maybe six and a half.
Axel Magnus: And when you notice the distress connected to that memory the image and the feeling what number comes up on a scale from zero to ten, zero being no disturbance and ten being the most disturbance you can imagine?
Client: Eight.
Axel Magnus: Eight. And the compressed weight below the sternum it’s there?
Client:(nods) Very much.
Intervention bilateral stimulation sets
Axel Magnus: Good. Hold the image of his face, the belief “I always mess things up,” and that compressed weight below your sternum all three together. And follow my hand. (begins bilateral hand movements, slow and steady)
[Approximately 28 passes. Axel observes: the client’s jaw tightens slightly at the start, then begins to loosen. A visible breath escapes around pass twenty. Hands shift from gripped on knees to resting open.]
Axel Magnus:(stops movement) Take a breath. Just let it go. And now without trying what comes up?
Client:(exhales) That was strange. I saw my father’s hands. Not his face. His hands on the broken pieces, trying to fit them back together. I didn’t remember that part.
Axel Magnus: His hands, trying to fit the pieces back. Stay with that. (bilateral stimulation resumes)
[Another set. The client’s brow softens measurably. Their shoulders drop a quarter inch.]
Client: It’s shifting. The weight… it’s still there, but it’s looser. Less compressed. And I’m noticing something weird I don’t think he was angry. I think he was sad.
Axel Magnus: He was sad. Stay with that. (another set)
[Client’s eyes redden slightly. Their breath becomes fuller visible expansion of the ribcage.]
Client: That changes things. I spent thirty years thinking he was angry at me. But in that memory, he just… looked heartbroken. About the model. Not at me.
Axel Magnus: Stay with that. (longer set)
[After this set, the client is visibly different a quality of stillness that was not present at the start. The bracing around the upper body has released.]
Client: The weight is much smaller. It’s still there, but it’s like… a remnant. And I notice my chest feels more open.
Axel Magnus: SUD now, zero to ten?
Client: Three. Maybe two and a half.
Axel Magnus:(continuing sets, shorter now) And the belief “I always mess things up” where is that now?
Client: It’s… less absolute. Like it was a rule I made from one moment, and I’ve been applying it everywhere since then.
[Two further sets. SUD reaches 1.]
Installation anchoring the positive cognition
Axel Magnus: Now I want you to bring in the positive cognition: “I handle things well enough.” Hold the original memory his expression, then his hands and the belief “I handle things well enough.” How true does that feel now, one to seven?
Client:(pause) Four. It feels more reachable than before.
Axel Magnus: Four. Good. (bilateral stimulation, steady sets) Stay with “I handle things well enough” and that memory.
[Two more sets. VoC climbs.]
Client: Five and a half. Almost six. There’s something in my chest now that warm feeling I described earlier. It’s showing up.
Axel Magnus: Stay with the warmth and the belief. (another set) VoC?
Client: Six. Close to seven. The warmth is spreading. It’s in my throat now too.
Axel Magnus: Good. Let it spread where it wants to go. (final installation set)
Client: Seven. That’s a seven. It feels real. Not just intellectual.
Body scan verifying somatic convergence
Axel Magnus: Excellent. Now I’d like you to scan from the top of your head to the soles of your feet, holding the original memory and the positive belief together. Tell me anything that feels unresolved any tension, tightness, or heaviness.
Client:(long pause, scanning visibly) There’s a small residual tightness in my throat. Like something unspoken.
Axel Magnus: Stay with the throat tightness. (short set)
Client:(afterward) It released. I had a flash of something I wanted to say to him, years ago, that I never said. Something like “I wanted you to be proud of me.”
Axel Magnus:(gently) And now?
Client: Now I think I know he was, in his own way. The tightness is gone.
Axel Magnus: Scan again, head to feet.
Client: Clear. Everything’s neutral. My chest is warm. I feel… settled.
Integration
Axel Magnus: Before we close notice where in your body you feel the settled quality most strongly right now.
Client: Sternum and upper chest. Where the weight used to be.
Axel Magnus: Good. That location now holds something different. You can return to that warmth and that settled feeling whenever you need it. Let’s take a few minutes before you leave, just breathing into that place.
[Three minutes of quiet breathing. The client leaves noticeably different in posture shoulders back, head carried more easily.]
💪 MEDITATION FOR EMDR AND SOMATIC BELIEF CHANGE
Find a position that feels comfortable seated or lying down, whatever allows your body to settle. And you might begin to notice, even now, as you read these words, that there is a quality of attention beginning to soften… a gentle turn inward that happens naturally, without effort, the way a leaf settles toward water…
Allow your eyes to close in their own time, and as they do… there may be a small release… a slight exhalation… and you might begin to notice the weight of your body against whatever is holding you… the chair, or the floor, or the bed… and how that support was always there, even when you forgot to notice it…
As you breathe… you might allow each breath to travel a little further than usual… down into the belly… as if your breath has been given permission to take up more space… and as it does… you may notice certain areas of the body beginning to soften… without you having to do anything at all…
Bring to mind a belief you carry about yourself… one of those quiet certainties that lives not in thought but in sensation… you don’t need to name it fully… just sense where it lives in the body… its location… its texture… perhaps a density, or a pressure, or a particular quality of heaviness that has been there so long you stopped noticing it…
And you might find it interesting to observe this sensation the way a curious scientist would observe something under a lens… not with judgment… just with genuine interest… where exactly is it?… what shape does it take?… does it have a temperature?…
And now… as you hold this awareness of the sensation… imagine two points of light… one on your left side… one on your right side… moving gently back and forth… back and forth… not urgent… not demanding… just a steady, rhythmic alternation, the way light moves across water in the late afternoon…
And as you follow this gentle movement… you might notice that the sensation in the body begins to change… not because you are forcing it… but because the nervous system knows how to update itself when given the right conditions… the way a dream resolves something the waking mind could not…
Perhaps the density shifts… loosens slightly… perhaps it moves… perhaps something unexpected arises alongside it an image, a memory, a sound, a warmth and whatever comes, you can allow it to pass through… like weather through an open window…
And as the movement continues… somewhere in your awareness… a different feeling may begin to take form… not manufactured… not performed… but real… a warmth in the chest, perhaps… or a steadiness somewhere in the torso… or an opening at the base of the throat… some quality that belongs to a belief more aligned with who you actually are…
And you might allow that feeling to grow at its own pace… to take up space… to move wherever it needs to move… the way warmth moves through the body when you step into sunlight after being cold…
Staying with that warmth… that steadiness… you might discover that somewhere in the body… a new truth has found a place to live… not just known… but felt… not just thought… but real… in the way the body makes things real, which is the only way that matters…
When you are ready… allow your awareness to expand gently… noticing the sounds in the room… the feeling of your breath… the weight of your body… and the quality that remains in your chest, or your belly, or your throat… carrying it with you as you return to full wakefulness… knowing that what has been planted here… continues to grow after you open your eyes…
🗣️ ANECDOTE ABOUT EMDR AND SOMATIC BELIEF CHANGE
Her name was Marta not her real name, but a name she chose herself when I offered her the choice in our first session. She was forty-three years old, a midwife, and she had spent the previous decade doing work she described as deeply meaningful while privately certain that she was incompetent.
“I know the facts,” she said in our first meeting. “I know my outcomes are good. I’ve been trained well, I have experience. But there is something right here “ she pressed a hand flat against her diaphragm “that doesn’t believe any of it. It’s like there’s a second voice underneath, running constantly: you’re pretending. Eventually they’ll find out.”
The somatic specificity was striking. She could locate the belief precisely. Not in her head in her body, at the level of the solar plexus, a sensation she described as a constant low-grade vibration, like a tuning fork always slightly off pitch.
Over three sessions, we worked through a cluster of memories connected to the core negative cognition “I am a fraud.” The earliest was not a dramatic event. It was a quiet one: age eleven, she had given a confident answer in class, been wrong, and watched her teacher’s expression move through a sequence surprise, then pity, then something she had read as confirmation. She had built a thirty-year architecture of self-doubt on that one expression.
By the third bilateral stimulation set of our second session, something shifted. She had been holding the image the teacher’s face and following the bilateral taps when she suddenly stopped.
“Wait,” she said.
I paused.
“I just realized I was right. I was right, and she misheard me. I remember now. She said ‘good guess’ and moved on, but I remember what I actually said. I was right.”
The room was very quiet.
“I’ve been carrying a wrong memory,” she said slowly, her hand moving to her diaphragm. “The vibration is still there. But it’s… different. Like it’s asking a question now instead of making a statement.”
By the end of that session, the VoC for “I am good enough at this” had moved from 2 to 5.5. The solar plexus had shifted from tuning fork to warmth. Not complete she was clear about that, and we both appreciated her precision but qualitatively different.
In our final session, during the body scan, she paused at her hands.
“My hands feel different. Steadier.”
“How long have your hands felt unsteady?” I asked.
“Ten years.”
She sat with that for a moment, and then she laughed a real laugh, surprised at herself.
“I have been delivering babies with unsteady hands for ten years.”
“And the outcomes were good.”
“And the outcomes were good,” she agreed. “Which means either I’m better than I thought, or the body somehow does what it knows even when the mind is arguing.”
I believe it is both. The body holds both the wound and the capability. EMDR helps it remember the capability was there all along.
👣 THE BASIC PROCESS OF EMDR AND SOMATIC BELIEF CHANGE
Step 1: Map the belief to its body location
Before beginning any formal protocol, spend time locating where the target belief lives physically. Ask: “When this belief is most active, where do you feel it in your body?” Invite specificity not just “my chest” but “a specific point two inches below my sternum, the size of a fist.” This somatic location will serve as your primary tracking point throughout the entire process.
What to notice: a particular quality of sensation pressure, heaviness, heat, constriction, or numbness. If you feel nothing, that absence is itself information worth tracking.
Step 2: Establish your parameters (assessment phase)
Identify the target image (the worst single moment connected to the belief), the negative cognition (phrased in first person: “I am helpless,” “I am broken,” “I don’t deserve…”), the positive cognition (what you would rather believe: “I have choices now,” “I am worthy,” “I am safe”), and your baseline measurements SUD from 0 to 10, and VoC from 1 to 7.
Write these down before starting. The numbers give you waypoints for tracking movement through the process.
Step 3: Establish dual attention
True bilateral stimulation requires holding two streams of attention simultaneously: the target memory, and present-moment sensory input. If you are working alone, you can use a bilateral audio track with alternating tones in each ear through headphones, combined with gentle self-tapping on alternating knees. The critical requirement is simultaneous activation of both hemispheres while the memory is held.
Step 4: Run the first processing sets
Activate the target image, negative cognition, and body sensation together. Begin bilateral stimulation (approximately 24-30 passes or taps). End each set with a blank screen: “Just notice. Whatever comes.” Then report to yourself or a partner what arose. A new image? A shift in sensation? An emotion? A thought? Feed whatever came up as the starting point for the next set.
Do not steer. Whatever the nervous system produces is part of the processing. Follow the material, not an agenda.
Step 5: Check SUD after every two or three sets
You are watching for a general downward trend. SUD may spike temporarily as the material is fully activated before it begins to resolve this is normal and expected. If SUD remains stuck or climbs sharply, slow down. Process a smaller fragment of the memory, or return to the body for grounding before continuing.
Step 6: Install the positive cognition
Once SUD has reduced to 0 or 1, shift from desensitization to installation. Pair the original target memory with the positive cognition and apply additional bilateral stimulation. After each set, check VoC. Continue until VoC reaches 7. Somatic confirmation: the positive belief should now produce a felt sense warmth, expansion, or steadiness somewhere in the body.
Step 7: Run the body scan
Scan from head to toe while holding the target memory and positive cognition simultaneously. Any residual charge tension, tightness, nausea, or a suspicious numbness indicates incomplete processing. Run additional bilateral sets focused on that location until the body returns neutral.
Step 8: Ground and close
End every session whether processing completed or not with grounding. Five slow breaths. Both feet on the floor. Notice five things you can see in the room. Brief body check: where do you feel most settled right now? Name that location internally and let the session end there.
▶️ VIDEO ABOUT EMDR
How EMDR Psychotherapy works in your brain
A concise animated explainer narrated by Esly Carvalho, Ph.D., that walks through the basic neuroscience of how EMDR works covering memory storage, the role of the amygdala, and why bilateral stimulation appears to facilitate adaptive memory reprocessing. Useful for both clients trying to understand the mechanism and practitioners looking for a clear overview to share.
The neuroscience of EMDR with Professor Paul Miller
A more in-depth video exploring the current neuroscience evidence behind EMDR from a research perspective. Professor Miller addresses how trauma memories differ from ordinary memories at the level of neural encoding, and why bilateral stimulation may facilitate the integration of fragmented somatic and narrative memory. Recommended for practitioners and researchers who want to go deeper into the evidence base.
Question: Is EMDR only for PTSD, or can it be used for general limiting beliefs?
Answer: EMDR was originally developed for PTSD, and its evidence base is strongest there. However, the protocol has been adapted for a wide range of presentations, including limiting beliefs that do not meet the full diagnostic criteria for PTSD. Many beliefs like “I am not enough” or “I can’t be trusted” are rooted in specific formative memories that respond well to the same processing protocol. The mechanism is the same: a fixed pattern in the nervous system that was established by an overwhelming experience and has never fully updated.
Question: How do I tell the difference between a genuine somatic shift and just relaxing during the session?
Answer: Genuine processing produces movement you notice changes in sensation, unexpected images arise, emotional quality shifts, or you access information you were not consciously aware of. General relaxation is pleasant but relatively static. A useful indicator is the associative quality: during processing, one thing leads to another in a way that feels almost self-generating. The nervous system is following a chain of associations. If you are simply feeling calmer without any of this movement, you may need to re-activate the target more fully before continuing.
Question: What if I process the same memory multiple times and it keeps coming back?
Answer: This usually indicates one of three things: the target memory is actually a network of related memories, and the presenting one is a branch rather than the root; there is a secondary memory with higher emotional charge that needs to be targeted first; or the positive cognition being installed is not ecologically sound something in the system is objecting because the new belief doesn’t yet feel safe to hold. Reevaluation at the start of each subsequent session is designed precisely to catch this.
Question: Can EMDR be done alone without a therapist?
Answer: For significant trauma abuse, accidents, combat, loss self-directed EMDR is not recommended. The therapeutic relationship provides a regulatory resource the nervous system uses during processing, and the absence of a skilled practitioner means there is no one to intervene if processing becomes destabilizing. For milder limiting beliefs with low SUD scores, some practitioners do work independently using bilateral audio and self-tapping, but the appropriate level of professional support depends on the material.
Question: Why does EMDR sometimes feel worse before it feels better?
Answer: Memory reprocessing often requires fully activating the material before the system can update it. The first few bilateral sets may temporarily intensify sensation or emotion as the memory is brought into full working memory. This is functionally similar to how an infected wound must sometimes be opened before it can heal. The SUD may climb before it falls. This is not a sign of failure it is usually a sign that the target has been correctly identified and processing has genuinely begun.
Question: How long does EMDR take to work?
Answer: Research consistently shows that single-incident trauma often resolves in three to six sessions. Complex developmental trauma where the belief system has multiple roots across different developmental periods requires longer, often many months of work. Somatic complexity adds time: a belief that has been held in the body for decades has structural correlates in posture, muscle tone, and nervous system regulation that update more slowly than episodic memory. Improvement is usually incremental and becomes more stable over time.
Question: Is the body scan at the end of a session necessary if I feel fine?
Answer: Yes. Feeling fine cognitively and emotionally does not guarantee that the somatic layer has fully updated. The body scan is the only way to verify this. Beliefs are not purely cognitive they are embodied schemas, and incomplete somatic updating is the most common reason for apparent progress that reverses under stress. The body scan takes three minutes. It is never a formality.
Question: What if no childhood memory comes up during assessment?
Answer: This happens, and it is useful information. It may indicate dissociation from early memory, which itself warrants attention, or it may mean the current-day activating situation is sufficient as a target without needing a historical anchor. EMDR can be run with the most recent activating event as the target memory. Associative processing will often reveal the earlier roots organically during subsequent sets.
😆 JOKES ABOUT EMDR AND SOMATIC BELIEF CHANGE
“My therapist told me EMDR would help me reprocess old trauma. I assumed we’d be talking. We ended up staring at her fingers for forty minutes. It worked. I haven’t trusted fingers since.” - Anonymous
“The Validity of Cognition scale goes from one to seven. At the start of my session, ‘I am worthy of love’ scored a one. By the end, it scored a five. Progress. My bank account still disagrees.” - Anonymous
“They said the body holds trauma. Nobody warned me that the body is holding trauma in my jaw, my left shoulder, the bottom of my right foot, and apparently my relationship with elevators.” - Anonymous
“EMDR is when a therapist helps your nervous system have the conversation your nervous system refused to finish in 1993.” - Anonymous
“My SUD went from nine to one during one session. Felt incredible. Then my brain said ‘hold on, we’re not done’ and sent me three related memories overnight. Turns out the unconscious works overtime and does not respect weekends.” - Anonymous
“Somatic belief change: finding out the thing you thought was your personality was actually just your body’s emergency posture that it forgot to turn off.” - Anonymous
🦋 METAPHORS FOR EMDR AND SOMATIC BELIEF CHANGE
The overactive smoke alarm: Imagine a smoke alarm that went off during a fire thirty years ago and was never reset. It now sounds for candles, toast, summer heat, any warmth at all. The alarm is not broken it was calibrated to a real emergency. EMDR does not remove the alarm. It recalibrates it to distinguish between genuine smoke and the smell of morning coffee. The body learns the difference, and the constant screaming quiets.
The stuck drawer: Old trauma beliefs are like a kitchen drawer that jammed at an odd angle and has been stuck ever since. The contents are still there they haven’t gone anywhere but the drawer neither fully opens nor fully closes. Every attempt to use it requires working around the jam, which eventually becomes so habitual you forget the drawer was ever meant to open easily. Bilateral stimulation is the precise jiggle that finally releases the catch. The drawer opens. You can reach what’s inside.
Sediment in a jar: Picture a jar of water with sediment at the bottom the undissolved residue of an old experience. The sediment is always there, muddying things whenever the jar is disturbed. EMDR does not pour the sediment out. It suspends the particles in motion long enough for the system to recognize them as part of the water rather than a foreign intrusion. Over time they disperse. The water clears.
The looped film reel: Traumatic memory often runs like a film reel caught in a loop the same frames repeating, the projector unable to advance to the next scene. Bilateral stimulation appears to act like a hand on the reel: it introduces just enough external rhythm to break the loop. The film begins to move forward again. Characters age. Stories reach their endings. The projector can finally turn off.
Rerouting a river: A belief held in the body for decades is a river that has carved its channel deep. You cannot fill in the channel with intention alone. EMDR works by introducing a new flow the bilateral stimulation, the present-moment sensory input that gradually widens an adjacent channel and allows the water to find a more adaptive course. Over sessions, the old channel narrows as it falls into disuse. The new one deepens.
Recalibrating a compass: A compass magnetized by a trauma event points consistently toward threat. It reads every room as a battlefield, every ambiguous expression as contempt, every uncertainty as catastrophe. EMDR does not destroy the compass you need it. It removes the distorting magnetization, so the needle can find true north again: what is actually here, now, in this room, as opposed to what was there, then, in that one moment.
🧑🦲 AXEL MAGNUS’S EXPERIENCE WITH EMDR AND SOMATIC BELIEF CHANGE
I came to EMDR sideways.
My background is not clinical. I trained as an aeronautical engineer before I understood that the most interesting engineering problem I would ever encounter was the one inside the person standing in front of me. By the time I was studying under Connirae Andreas and working with the Core Transformation and Wholeness Process methodologies, I had already spent years as a yoga instructor, a mentalist, a practitioner of somatic approaches to change. I had catalogued hundreds of body sensations and watched them shift in session after session. I thought I understood the body’s role in belief change.
And then someone explained EMDR to me, and I realized I had been working around an entire territory without knowing it existed.
My first encounter with bilateral stimulation was not as a client. It was a demonstration someone in a training showed me the alternating tapping, explained the working memory hypothesis, ran through the phases. I sat there with my engineer’s mind asking: but what is actually happening in the nervous system? I went home and read for three days straight. What I found in the neuroimaging literature was not what I expected. The changes were not soft they were structural. Measurable. Grey matter. Amygdala activity. Prefrontal engagement. The body was being literally reorganized.
I decided to experience it myself.
The belief I chose to work on was not dramatic. It was quiet and persistent: “I understand things better when I observe them from a distance.” On the surface it sounded like a personality trait, even a virtue. Underneath it was a belief about the danger of being close close to people, close to my own experience, close to anything that might be lost. Distance was safety. I had been running this belief since childhood, and it had served me in certain ways: I became good at seeing patterns, at reading rooms, at understanding systems. I also became very good at being peripheral.
The session ran for ninety minutes. I remember the moment around the fourth set of bilateral taps when something unexpected rose up. Not the memory I had targeted. An image of my hands. My child’s hands, very specifically, reaching toward something and then pulling back. Reaching and pulling back. The hands did not know what they wanted. They only knew the pulling back was safer.
I felt something in my chest then that I can only describe as a long-overdue recognition. Not sadness, exactly more like the feeling of returning to a room you left decades ago and finding it exactly as you left it, everything preserved in the amber of an old decision.
By the end of the session, the belief had not disappeared. Beliefs installed over decades do not vanish in ninety minutes. But the quality had changed: from a certainty to a question. “Do I actually still need this?” The sensation in my chest which had been a kind of careful hollowness was warmer. More inhabited.
What has stayed with me most is this: the body knew something the mind had been successfully avoiding for thirty years. The bilateral stimulation did not create new information. It simply created the conditions in which information the body had been holding quietly could finally be heard.
I now incorporate the principles of iterative, bilateral processing combined with somatic tracking and NLP submodality work into my practice routinely. What EMDR taught me is that lasting belief change requires full somatic participation. Everything else is negotiation with the surface.
🕳️ THE LIMITATIONS OR UNCERTAINTIES IN EMDR AND SOMATIC BELIEF CHANGE
EMDR is not a universal solution. For some people and some presentations, EMDR produces little movement. Individual differences in dissociative capacity, attachment style, and nervous system regulation affect how readily the protocol works. For those with highly dysregulated nervous systems, extensive preparation building somatic resourcing and window of tolerance is often required before any memory processing can safely begin.
Contraindications require careful assessment. Active psychosis, severe dissociative disorders without specialist support, significant self-harm risk, and major medical instability are among the presentations where standard EMDR protocol requires significant modification or is contraindicated. Working with complex trauma should only be done under qualified clinical supervision.
The mechanism is still debated. Numerous hypotheses exist for why bilateral stimulation works the working memory hypothesis, the orienting response model, the interhemispheric integration account, the Adaptive Information Processing framework developed by Shapiro herself. None of these has been definitively established. The clinical outcomes are well supported by research; the mechanism remains an open question.
Cultural considerations matter. The experience of trauma, the meaning of somatic sensation, the appropriate relationship between practitioner and client, and the cultural frame for discussing distress vary enormously. EMDR was developed in a Western, largely individualist therapeutic context. Its assumptions about disclosure, about the therapeutic relationship, and about what constitutes resolution may not translate directly across cultural settings.
Positive cognitions must be ecologically sound. If the nervous system object to a positive cognition for legitimate reasons if “I am safe” is not actually true in the client’s current environment installation will fail or produce confusion. EMDR is a tool for updating the nervous system’s relationship to past experience. It cannot and should not override an accurate threat assessment in the present.
Processing can temporarily increase distress. In the days following an EMDR session, as the brain continues processing material uncovered during the session, some clients experience heightened emotional sensitivity, vivid dreams, or the surfacing of additional memories. This is usually temporary and is a sign of active integration rather than deterioration but it requires psychoeducation, adequate aftercare, and clear access to support.
Self-directed EMDR carries significant risks for complex trauma. While bilateral audio tools and self-tapping protocols are widely available online, using them without professional support to process significant developmental trauma is not recommended. The regulatory function of the therapeutic relationship is not a luxury it is a core component of why EMDR works, and its absence changes the risk profile substantially.
✏️ CONCLUSION
The body does not lie, but it can be wrong. This is the strange double truth at the center of somatic belief change: every sensation is real, every tension genuine, every pattern of bracing or withdrawal meaningful and yet the interpretation the body is running may be decades out of date.
EMDR works because it goes to where the outdated interpretation lives. Not the narrative layer, where we can talk ourselves into almost anything temporarily, but the somatic layer, where the old belief has been dutifully maintaining its watch since the moment it was installed. The eight phases of the protocol are a structured way of meeting the nervous system on its own terms, in its own language sensation, image, prediction error, bilateral rhythm and inviting it to update.
What emerges after that update is not a different person. It is the same person, freed from a particular architecture of self-protection that once made complete sense and no longer does. The compressed weight below the sternum loosens. The hands relax. The breath travels all the way down. The body discovers, sometimes with something close to surprise, that it can hold a new truth and that the new truth fits better.
That is the aim. Not certainty. Not perfection. Just a nervous system that has been given a chance to catch up with what is actually true, here, now, in this body, in this life.
📚 REFERENCES
George Lakoff & Mark Johnson, 1980; Metaphors We Live By
Steve & Connirae Andreas, 1987; Change Your Mind and Keep the Change: Advanced NLP Submodalities Interventions
Julian Jaynes, 1976; The Origin of Consciousness in the Breakdown of the Bicameral Mind
Andreas, S. (2002). Transforming yourself: Becoming who you want to be. Real People Press.
Connirae Andreas & Steve Andreas, 1989; Heart of the Mind: Engaging Your Inner Power to Change with Neuro-Linguistic Programming
Connirae Andreas & Tamara Andreas, 1994; Core Transformation: Reaching the Wellspring Within
Video DVD Transforming Yourself: Complete 3-Day Training with Steve Andreas
Shapiro, F. (1989). Eye movement desensitization: A new treatment for post-traumatic stress disorder. Journal of Behavior Therapy and Experimental Psychiatry, 20(3), 211–217.
van der Kolk, B. (2014). The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. Viking.
Levine, P. (1997). Waking the Tiger: Healing Trauma. North Atlantic Books.
Shapiro, F. (2001). Eye Movement Desensitization and Reprocessing: Basic Principles, Protocols, and Procedures (2nd ed.). Guilford Press.
Lansing, K. et al. (2005). High-resolution brain SPECT imaging and EMDR in police officers with PTSD. Journal of Neuropsychiatry and Clinical Neurosciences.
Eternal Sunshine of the Spotless Mind (2004) explores the idea of selectively erasing painful memories and the complex relationship between memory, identity, and emotional healing
Ordinary People (1980) a closely observed portrayal of trauma processing, survivor’s guilt, and the work of therapeutic change
Good Will Hunting (1997) depicts the gradual dismantling of a deeply held negative self-belief through the therapeutic relationship
📺 TV SHOWS ABOUT EMDR AND TRAUMA BELIEF CHANGE
In Treatment HBO series following week-by-week therapy sessions; several storylines explore body-held trauma and belief reorganization
Mindhunter explores the psychology of deeply embedded belief systems and how they form and persist
The Affair structured around competing subjective memories of the same events, illuminating how the same experience can be encoded differently in different nervous systems
🎭 DOCUMENTARIES ABOUT EMDR AND TRAUMA BELIEF CHANGE
Heal (2017, Netflix) examines evidence-based and alternative approaches to mind-body healing, including trauma treatment
The Wisdom of Trauma (2021) Gabor Maté’s documentary on how trauma shapes identity, health, and the body’s encoding of experience
Free the Mind (2012) documents the use of mindfulness and EMDR-adjacent techniques with combat veterans and children with anxiety disorders
📚 NOVELS ABOUT EMDR AND TRAUMA BELIEF CHANGE
The Body Keeps the Score by Bessel van der Kolk (2014) while technically non-fiction, it reads with narrative depth and is the most comprehensive lay account of how trauma is somatically encoded and how EMDR contributes to its resolution
The Shock of the Fall by Nathan Filer a first-person account of grief, guilt, and the fragmented nature of traumatic memory
A Little Life by Hanya Yanagihara a deeply demanding but precise literary exploration of how early trauma embeds itself as identity and the limits of therapeutic repair